Answer Key
to 2003 Exam
Course Directors:
Pathology Pathophysiology Pharmacology
Calvin Oyer, M.D. Douglas Burtt, M.D. Robert Patrick, Ph.D
Questions 1 – 8: A twenty eight year old white male is brought
to the Emergency Room after an episode of syncope (transient loss of
consciousness) while playing basketball. Physical examination reveals a bifid
carotid pulse and a mid-peaking systolic murmur which accentuates with standing
up or Valsalva maneuver.
Answer C: This patient has hypertrophic cardiomyopathy
with obstruction, and has hypernormal
1. This patient would
be expected to have all of the following echocardiographic findings, except:
A) systolic anterior motion of the mitral valve leaflets
B) a normal appearance of the aortic valve
C) left ventricular systolic dysfunction
D) disproportionate upper septal thickening
E) diastolic left ventricular dysfunction
Answer D: Treatment of this condition is aimed at either
mechanical reduction of the upper septal obstruction or medication aimed at
relaxing the ventricle in diastole, to improve
2. Subsequent treatment of this patient might include each of
the following, except:
A) Surgical resection of a portion of the upper intraventricular septum
B) Alcohol septal ablation of a localized area of the upper septum
C) Medical therapy with a calcium channel blocker
D) Medical therapy with digoxin
E) Medical therapy with a beta blocker
B: Both of these drugs are beta-blockers, but propranolol is non-selective and would affect the lung
by exacerbating bronchoconstriction. All beta
blockers inhibit the effect of beta agonists on the heart.
3. In comparing propranolol to
atenolol, all of the following statements are correct EXCEPT:
A. Both drugs can be used to treat hypertrophic
cardiomyopathy
![]()
B. Propranolol would be preferred for usage in a patient with asthma
C. Neither drug blocks catecholamine alpha-1 receptors
D. Both drugs inhibit norepinephrine-induced stimulation of cyclic AMP production in the heart
E. Both drugs block catecholamine beta-1 receptors
4. This patient’s syncope may have been caused or contributed to by any of the following, except:
A: The syncope was most likely due to reduced preload
from dehydration coupled with increased systolic contractile force, both of
which would lead to increased outflow gradient and reduced systolic blood
pressure. Ventricular arrhythmias are more common in this condition and can
cause sudden death.
A) severe
hypertension due to increased
B) dehydration
worsening the
C) a transient ventricular arrhythmia (e.g. ventricular tachycardia)
D) adrenergic stimuli leading to increased outflow tract obstruction
E) decreased cardiac output secondary to a decreased stroke volume
5. A cardiac catheterization is performed, and a pullback pressure tracing starting at the apex of the left ventricle is made. Identify which tracing is associated with this patient’s condition:
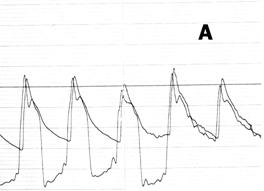
B: This is a classic pullback tracing for hypertrophic
CM with outflow obstruction, demonstrating the intra-ventricular gradient
between the apex of the heart and the area under the aortic valve. There is
no gradient between the aorta and the area just under the aortic valve.
Picture A is a normal pullback. Picture C is a patient with aortic stenosis.
 6. Gross pathological examination of the
myocardium of a patient with the same condition is shown here. All of the
following statements regarding this patient’s heart are true except:
(5 points)
6. Gross pathological examination of the
myocardium of a patient with the same condition is shown here. All of the
following statements regarding this patient’s heart are true except:
(5 points)
A. There was severe left ventricular outflow tract obstruction
B. He carried an increased risk for sudden death
C. The ratio of the thickness of the septum to the thickness of the left ventricular free wall is greater than 1.3/1
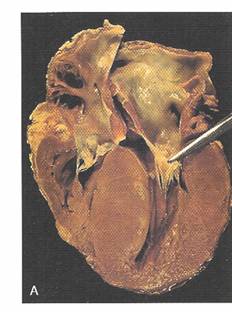
D. The compliance of the left ventricle was greater than normal
E. Microscopic examination would show large hyperchromatic nuclei in the myofibers and focal areas of myofiber disarray
D: The classic findings in this condition include
reduced compliance, as well as A,B, C and E.
7. Two diastolic filling curves are shown in figure 1. At which of the labeled points was this patient most likely to have been at the time of his syncopal episode?
Answer: A This is a tough
question….but…. this patient has a steeper compliance curve than normal,
limiting the choices to A and B. He most likely lost consciousness due to
reduced preload from relative dehydration and increased outflow tract
obstruction – at point A.
8. Two Frank-Starling relationships are shown in figure 2. At which of the labeled points on these curves was this patient most likely to be at the time of his syncopal episode?
Answer C: Another
toughie – again this patient has a Starling curve that is shifted up and to
the left, due to increased contractility. His cardiac output is decreased
due to reduced preload and he is therefore at point C.
Questions 8 – 13: A 57 year old female develops progressive dyspnea on exertion several weeks after a prolonged viral upper respiratory illness. She also notes fatigue, orthopnea and PND. An echocardiogram confirms a markedly dilated and hypocontractile left ventricle, with a left ventricular ejection fraction of 20%.
She presents to the hospital with worsening shortness of breath.
9. At which of the labeled points in figure 1 above (diastolic filling curves) was this patient most likely to be at the time of admission to the hospital?
Answer B: This patient has a dilated cardiomyopathy and
reduced
10. At which of the labeled points in figure 2 above (Frank-starling curves) was this patient most likely to be at the time of admission to the hospital?
E – This patient has an abnormal, flattened Starling
curve, shifted down and to the right, but is not in cardiogenic shock, and
therefore is not on the bottommost curve. (She is walking and talking, but
is short of breath.) At the time of presentation she is in CHF, and
therefore is in the upper right quadrant, on the middle curve, at point E.
B. Reduces aldo levels.
11. As part of her
treatment, this patient received an ACE-inhibitor, enalapril.
All of the following statements concerning enalapril are correct, except:
A. It may produce a persistent dry cough as a side
effect
![]()
B. It produces an increase in circulating aldosterone levels
C. It produces a decrease in vascular resistance
D. It inhibits the formation of angiotensin II
E. It should not be used in pregnant women
D: Of the three inotropic drugs on this list, Dig, Amrinone
and Dobutamine, Dig is the only one that works by the above mechanism.
12. As additional pharmacologic
therapy, this patient received an inotropic drug. Indicate which of the following drugs produces an inotropic effect
via inhibition of the cardiac Na+/K+-ATPase:
A. Captopril
B. Furosemide
C. Dobutamine
D. Digoxin
E. Amrinone
 13. Gross pathological examination of a similar
patient’s heart is shown in this photo of the open left ventricle
:
13. Gross pathological examination of a similar
patient’s heart is shown in this photo of the open left ventricle
:
The thickness of the
A. Idiopathic dilated cardiomyopathy
B. Longstanding essential hypertension, poorly controlled
C. Prolonged alcoholism and deficiency of intake of thiamine
D. A mother without history of previous heart disease who developed congestive heart failure 2 weeks postpartum
E. A 21 year old man with recent adenoviral infection who died suddenly while sleeping
B: Classic example of dilated cardiomyopathy, with
cavity dilation and little or no
Questions 14 – 20: A 64 year old black male presents to the hospital nearly 24 hours after the onset of severe substernal chest pressure. Physical examination reveals a heart rate of 110/minute, a blood pressure of 80/50, jugular venous distention, rales two thirds of the way up the lung fields and an S-3 gallop on cardiac exam. The EKG reveals sinus tachycardia at 110/minute with Q waves and ST segment elevations in the anterior leads.
14. At which point on the Frank-Starling curves in figure 2 would this patient be?
Point B, unfortunately. This
patient is in cardiogenic shock, with reduced blood pressure and elevated
filling pressures (CHF). His starling curve is shifted way down and is very flattened. He is in the lower right quadrant, consistent with
cardiogenic shock.
B: Large MI, leading to markedly reduced systolic
function, educed stroke volume, reduced cardiac output. No RV infarction
since this only occurs with inferior MIs. Too early for free wall rupture.
15. The
most likely cause of this patient’s hypotension is:
A) increased vagal tone
B) decreased stroke volume due to large anterior MI
C) vasodilation in compensation for the rapid heart rate
D) right ventricular infarction causing decreased preload
E) acute left ventricular free wall rupture
A Swan-Ganz right heart catheter is place in the patient, revealing the following:
RA pressure: 15 mm Hg
PA pressure: 50/30 mm Hg
PC wedge pressure: 30 mm Hg with normal V-waves
Cardiac output: 3 liters/minute (Cardiac index ~ 1.6 lit/min/m2)
D: Patients in cardiogenic shock from acute MI have a
dismal prognosis when treated medically. With emergency intervention (such
as angioplasty or stent) the mortality may be reduced to 50% or less.
16. Based on this
patient’s hemodynamic profile, his survival rate treated medically is:
A) greater than 90%
B) 70 - 80%
C) 40 - 50%
D) 10 - 15%
17. True statements about this patient’s biochemical markers and pathological findings include all of the following, except:
A) Serum CPK enzymes are likely to be significantly elevated
B) Histological inspection would be likely to demonstrate coagulation necrosis
C) Serum troponin I would not be likely to be significantly elevated yet
D) Gross pathological inspection of the heart would likely reveal a purplish discoloration at the site of infarction
E) CPK enzymes would continue to remain elevated for at least 48 hours
C – All cardiac marker enzymes would be elevated by 24
hours, and the ventricle would appear purplish and bruised, due to
coagulation necrosis. Enzymes would remain elevated for 48 to at least 72
hours.
Shortly after arrival to the hospital, the patient develops atrial fibrillation.
18. The pathophysiological mechanism of this arrhythmia is most likely:
- increased automaticity in the atrium
- increased automaticity in the A-V node
- increased conduction through the A-V node
- multiple areas of re-entry within the A-V node
- multiple areas of re-entry within the atrium
E – A fib is due to multiple areas of “micro-reentry”
within the atrium.
19. Digoxin can be used to treat atrial fibrillation because of its ability to:
C: Dig increases parasympathetic input and slows
conduction through the AV node, reducing the ventricular response rate –
thereby improving
A. Inhibit monoamine oxidase
activity in the heart
![]()
B. Inhibit catecholamine reuptake in the heart
C. Increase parasympathetic input to the heart
D. Inhibit cyclic AMP metabolism in the heart
E. Stimulate cyclic GMP production in the heart
20. Indicate which of the following drugs would be the most appropriate for the treatment of this patient’s hypotension and CHF:
E – Dobutamine is a rapidly acting iintravenous
inotropic agent which may improve heart failure
and blood pressure in cardiogenic shock. Because of a mild vasodilatory effect, however, the net effect on blood
pressure is usually small.
![]()
A. Isosorbide
B. Propranolol
C. Amiodarone
D. Neostigmine
E. Dobutamine
Questions 21 – 23: A 75 year-old female has been under treatment for arthritis with four weeks of non-steroidal anti-inflammatory drugs. She now notes two days of increasing chest pressure with exertion and black, tarry stools. On examination she appears pale and her vital signs are: Pulse 110/min; BP: 90/60; Resp: 16; Temp: 98.6 F.
21. Pathophysiologic mechanisms for her accelerated angina pectoris might include all of the following, except:
- Increased myocardial oxygen demand due to sinus tachycardia
- Increased left ventricular wall tension due to increased preload
- Increased myocardial contractility due to increased sympathetic tone
- Decreased diastolic coronary perfusion pressure due to hypotension
- Decreased
oxygen carrying capacity due to anemia
B: This patient
has tachycardia – increased oxygen demand; increased sympathetic tone –
increased contractility and increased demand; low diastolic BP – decreased
supply; anemia – decreased supply. But preload is reduced due to
anemia/volume depletion from recent GI bleeding.
22. During episodes of chest pressure, all of the following pathophysiologic mechanisms may be taking place, except:
A. increased local adenosine levels, causing local vasodilation (to increase coronary blood flow)
B. increased local EDRF or nitric oxide levels, causing local vasodilation (to increase coronary blood flow)
C. increased catecholamine production, causing increase in heart rate and contractility (increasing myocardial oxygen demand)
D. increased external compression of the coronary vessels, causing increased coronary vascular resistance
E. increased local cyclic-AMP levels, causing local vasoconstriction (decreasing coronary blood flow)
Answer E – Byproducts of cellular metabolism generally
lead to vasodilation, in order to increase myocardial blood flow.
23. Part of the medical treatment of this patient included long-acting nitrate therapy. All of the following statements regarding nitrate therapy are true, except:
A) Tolerance may develop to long-term nitrate therapy
B) Nitrates
reduce
C) Nitrates can cause hypotension, especially in volume-depleted patients
D) Nitrates cause coronary vasodilation, augmenting coronary blood flow
E) Nitrates increase levels of intra-coronary nitric oxide (EDRF)
This question was in error! All of the above statements
regarding nitrates are true, so we won’t count this question in the
grading!
![]() Questions 24 – 30: A middle
aged male patient with stable angina is found to have markedly elevated total cholesterol
and elevated serum triglycerides. Treatment with dietary modification as well
as pharmacologic therapy is advised.
Questions 24 – 30: A middle
aged male patient with stable angina is found to have markedly elevated total cholesterol
and elevated serum triglycerides. Treatment with dietary modification as well
as pharmacologic therapy is advised.
24. This patient is recommended by his physician to start a cardiac prudent diet. Components of this diet should include:
-
A diet high in n-6 polyunsaturated fats.C
- Less than 7% of calories total fat diet with multivitamin, flaxseed, and fish oil supplements.
- A diet rich in fruits and vegetables, fish and nuts.
- Low carbohydrate, Atkins type diet.
25. After placing this patient on a low saturated fat, low cholesterol diet, his serum total and LDL cholesterol both increase. The most likely explanation of this is:
A)
B
Regression to the mean
B) Genetic polymorphism
C) Compensatory raising of serum cholesterol due to lowering of serum HDL cholesterol
D) Saturated fats in diet replaced with carbohydrates which increases total and LDL cholesterol
26. This patient is recommended to increase his fish intake by his physician. The most plausible mechanism by which this dietary change may reduce the patient’s risk of a second coronary event is:
D
A) Lowers oxidized LDL cholesterol in the atherosclerotic plaques
B) Lowers serum LDL cholesterol
C) Increases expression of leukocyte adhesion molecules in atherosclerotic plaques
D) Promotes nitrous oxide induced endothelial relaxation
27. Simvastatin lowers plasma cholesterol via:
A. Binding bile acids
B. Stimulation of lipoprotein lipase activity
C
C. Inhibition of HMG-CoA reductase activity
D. Stimulation of cholesterol excretion
E. Inhibition of lipolysis, resulting in a reduction of free fatty acids
28. Indicate which of the following would have the greatest efficacy for lowering blood
triglyceride levels:
A
A. Gemfibrozil
B. Niacin
C. Atorvastatin
D. Ezetimibe
E. Colesevelam
29. A major toxicity associated with the statin drugs (e.g., lovastatin):
A. Hypotension
B
B. Myositis
C. Bladder cancer
D. Lowered white blood cell count
E. Male sterility
30. A lipid-lowering drug that inhibits lipolysis in adipose tissue is:
A. Simvastatin
D
B. Probucol
C. Gemfibrozil
D. Niacin
E. Colesevelam
Questions 31 – 35: Match each question with the single best answer (A - E)
|
31. Decreased diastolic aortic pressure; increased left ventricular end-diastolic pressure; volume overload of the left ventricle; bounding peripheral pulses |
CAortic Regurgitation |
|
32. Impaired diastolic filling of ventricles; Elevated jugular venous pressure with rapid
"y-descent"; left ventricular diastolic pressure tracing with "dip
and plateau" configuration |
A Constrictive Pericarditis |
|
33. Impaired diastolic filling of ventricles; cyclical decrease in systolic blood pressure during
inspiration; elevated jugular venous pressure without Kussmaul’s sign |
DCardiac Tamponade |
|
34. Impaired diastolic filling of the left ventricle; normal left ventricular end-diastolic pressure; increased pulmonary venous pressure with occasional
"reactive" pulmonary hypertension |
EMitral Stenosis |
|
35. Impaired diastolic filling of the ventricles; fibrosis,
scarring, or infiltration of the myocardium; normal pericardial
tissue |
B Restrictive
Cardiomyopathy |
36. The AV node is a requisite component of the reentrant circuit in:
a. Atrial fibrillation
C
b.
Atrial flutter
c. Orthodromic tachycardia associated with Wolff-Parkinson-White Syndrome
d. Ventricular tachycardia following remote myocardial infarction
e. Intra-atrial reentry
37. The majority of the duration of the PR interval reflects conduction through the:
a.
Sinus node
C
b. Atrium
c. AV node
d. His bundle
e. Purkinje system
38. The current responsible for depolarization of atrial and ventricular myocardial cells is carried predominantly by which ion?
a. Sodium
A
b. Potassium
c Calcium
d. Magnesium
e. Lithium
39. The current responsible for depolarization of sinus and AV node cells is carried predominantly by which ion?
a.
Sodium
C
b. Potassium
c. Calcium
d. Magnesium
e. Fluoride
in
40. A 72 year old female presents to the doctor’s office with exertional dyspnea and is found to have a systolic murmur consistent with mitral regurgitation (MR). The following statements regarding chronic and acute MR are all correct, except:
A – Classically, acute MR occurs with a normal
sized LA, hence the markedly elevated LA pressure with giant V-waves. In
contrast, chronic MR leads to an enlarged LA with normal or near normal
pressures.
A. Acute MR is associated with a larger left atrium than chronic MR
- Acute MR is associated with a higher left atrial pressure than chronic MR
- Acute MR has a harsher, less holosystolic murmur than chronic MR
- Acute MR is associated with recent inferior myocardial infarction, while chronic MR is not
- Both acute and chronic MR can lead to atrial fibrillation due to left atrial stretch
Match the ischemic syndrome with pathological findings.(each answer 3 points)
41. Acute plaque
changes with occlusive coronary thrombosis --
ANSWER B
![]()
42. Plaque erosion or rupture with microthrombi and microemboli --- ANSWER C
43. Fixed lesions with at least one lesion showing 75% or greater cross-sectional area reduction of lumen – ANSWER A
A. Stable angina pectoris
B. Myocardial infarction
C. Unstable angina pectoris
Match the occluded
coronary artery with the area of
infarction or clinical event. (each answer 3
points)
![]()
44. Right coronary artery in a right dominant system – ANSWER C
45. Left main coronary artery – ANSWER A
46. Proximal left anterior descending coronary artery – ANSWER B
A. Global dysfunction of the left ventricle
B. Anteroseptal infarct
C. Posterior wall infarct
Are the following developments normal (A) or abnormal (B)? (each answer 3 points)
47. L-loop of the ventricles. -- ABNORMAL
![]()
48.
Partial involution of the left horn of the sinus venosus
--
and persistence of a portion to form the coronary sinus.
49. Closure of the ductus arteriosus at the onset of labor. -- ABNORMAL
50. Migration of cells from the neural crest to participate in the formation of the
Conotruncus. --
51. All of the
following adaptive changes in the
myocardium would be expected in the presence of significant aortic stenosis, except: (3 points)
![]()
A. Increase in length and diameter of myocardial fibers
B.
C
Additional sarcomeres
C. Decreased messenger RNA and contractile proteins
D. Increase in size of myocyte nuclei with increased DNA content
E. Increase in number of mitochondria
Match the time after onset of myocardial infarction with the histological features/clinical event .(each answer 3 points)

52. Coagulation necrosis, wavy fibers, early nuclear changes, infiltration of the interstitium by a few polymorphonuclear leukocytes -- B
53. A scar with dense collagen fibers -- D
54. Thrombotic coronary artery occlusion with no histopathology in the myocardium -- A
55. Rupture of ventricular wall with cardiac tamponade -- C
A. 2 hours
B. 12 hours
C. 4-7 days
D. 6 weeks
56. Relative to fibrinous pericarditis, all of the following are true, except: (3 points)
A.
It can occur a few days after a transmural
acute myocardial infarct and usually is associated with a friction rub
![]()
B.
B
It is due to spread of tuberculosis from the mediastinum
C. Histology shows an inflammatory reaction and deposition of fibrin
D. It is unlikely to be followed by constrictive pericarditis
The histological diagnosis of myocarditis
requires the presence of 2 features. For each of the choices below, choose True (A) or False (B). (3 points)
![]()
57. Myocardial damage as shown by myocyte necrosis, myocyte dropout, or myocytolysis -- TRUE
58. Recent intake of a drug known to cause myocarditis -- FALSE
59. An interstitial infiltrate of inflammatory cells -- TRUE
60. The presence of giant cells -- FALSE
Questions 61 – 67: True (A) or False (B) (each answer 3 points)
61. Wegener’s granulomatosis is a large vessel vasculitis in which a test for p-ANCA is likely to be positive. -- FALSE
62. Hyaluronate in the wall of group A streptococci is identical to that in human connective tissue -- TRUE
63. The Aschoff body consists of an area of fibrinoid degeneration surrounded by lymphocytes, plasma cells, large macrophages, and giant cells. -- TRUE
64. The predominant type of lymphocyte found in the infiltrate in viral myocarditis is the B cell. -- FASLE
65. A patient undergoes thrombolysis 2 hours after coronary occlusion. There is a possibility of salvage of some myocardium. The preserved area will be subepicardial. -- TRUE
66. A myocardial infarct occurring as a result of prolonged shock in a young accident victim with no significant coronary disease is usually transmural and in the zone of a specific coronary artery branch. -- FALSE
67. BNP, a test for the level of brain natriuretic peptide in serum, is useful in differentiating dyspnea due to lung disease from dyspnea due to heart failure. -- TRUE
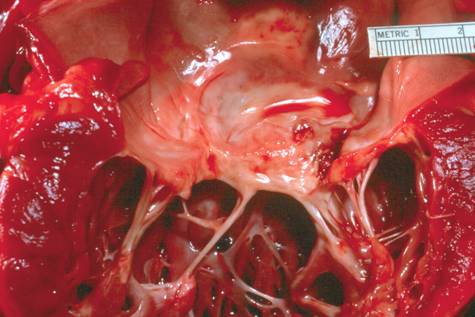 68.
This is a view of the mitral valve from the open left atrium. The most likely
scenario to explain this severe deformity is: (5 points)
68.
This is a view of the mitral valve from the open left atrium. The most likely
scenario to explain this severe deformity is: (5 points)
A. The patient had undergone a surgical procedure to repair papillary muscle rupture
B. The patient has noted dyspnea on exertion, has increased stroke volume, left ventricular dilation, and a prominent holosystolic murmur at the apex
C. There is a history of streptococcal pharyngitis with fever and subsequent joint pain and swelling in childhood and the patient has now been experiencing orthopnea and paroxysmal nocturnal dyspnea
D. The patient also has aortic root dilation and a family history of Marfan syndrome
E. The patient had recently migrated from
C – A classic case (I’m told) of rheumatic valvular
deformity with shortening and thickening of the chordae
and sub-mitral apparatus. Always due to rheumatic fever (well – almost
always)!
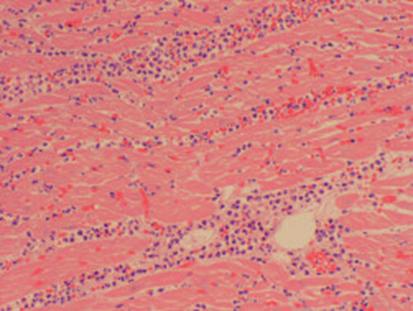 69. Choose the correct statement about this microscopic
section of myocardium. The infiltrating cells are neutrophils.
(5 pts)
69. Choose the correct statement about this microscopic
section of myocardium. The infiltrating cells are neutrophils.
(5 pts)
A. This ventricular wall carried a great risk for rupture
B. It represents an area of infarction in which the onset of symptoms was approximately 2 days prior to death
C. The patient almost certainly had a transient right bundle branch block
D. It is from a child who recently had an adenoviral infection
E. The patient traveled in
B – Recent myocardial infarction with infiltration of neutrophils, but not yet at the point of yellow
softening.
70. All of the following statements are true except: (5 points)
 A.
There is an anteroseptal infarct with onset about 24
hours prior to death
A.
There is an anteroseptal infarct with onset about 24
hours prior to death
B. There is an anteroseptal infarct with onset about 5 days prior to death
C. There was risk of rupture of the ventricular wall and/or the ventricular septum
D. There was a possibility of formation of a ventricular aneurysm if the patient survived
E. Microscopic study would show macrophages and early granulation tissue
A – This is an anteroseptal MI
about 4 – 7 days old, with yellow softening and a change in the
inflammatory cells to macrophages and early granulation tissue. Prone to rupture or aneurysm formation.
 71.
The following statements about the
aortic valve pictured above are all true, except: (5 points)
71.
The following statements about the
aortic valve pictured above are all true, except: (5 points)
A. The underlying anomaly is one of the most frequently encountered congenital cardiac defects
B. The valve pictured above has undergone thickening of the cusps and is stenotic
C. The problem is probably compounded in this case by severe mitral stenosis
D. This type of anomaly is often associated with coarctation of the aorta
E. This patient probably had concentric left ventricular hypertrophy
C – Typical bicuspid aortic valve leading to aortic
stenosis and concentric LVH. Most common congenital
abnormality.
72. The potency of a drug is defined as:
A. The minimal concentration of a drug needed to produce a physiological response
C
B. The concentration of a drug needed to produce a maximal
effect
C. The concentration of a drug needed to produce 50% of the maximal effect
D. The maximal physiological effect that can be achieved with the drug
E. The minimal concentration of a drug needed to counter the effect of a competitive inhibitor
73. The efficacy of a drug is defined as:
E
A. The concentration of a drug needed to produce a maximal
effect
B. The minimal concentration of a drug needed to counter the effect of a non-competitive inhibitor
C. The minimal concentration of a drug needed to produce a physiological response
D. The concentration of a drug needed to produce 50% of the maximal effect
E. The maximal physiological effect that can be achieved with the drug
74. In the presence of a competitive receptor antagonist the following will be observed with regard to binding of the agonist to the receptor:
B
A. An increase in the Kd and an increase in
the Bmax
B. An increase in the Kd and no change in the
Bmax
C. No change in the Kd and a decrease in
the Bmax
D. A decrease in the Kd and a decrease in
the Bmax
E. An increase in the Kd and a decrease in
the Bmax
75. Drug A has an TD50 of 6 mg/kg and a Therapeutic Index (TI) of 30. What is the ED50 of Drug A?
E
A. 180 mg/kg
B. 5 mg/kg
C. 2 mg/kg
D. 0.5 mg/kg
E. 0.2 mg/kg
76. The following will occur when “spare receptors” are present:
A. The receptors will only respond to maximal concentrations of agonist
D
B. Receptor binding will not saturate as the agonist concentration
is increased
C. Only non-competitive inhibitors, but not competitive inhibitors, will be able to inhibit agonist binding
D. The ED50 will have a lower value compared to the Kd
E. All of the above
77. At opiate receptors, heroin is a full agonist and buprenorphine is a partial agonist. This means that:
A
A. Heroin will have a greater efficacy compared to buprenorphine

B. Heroin will have a lower ED50 compared to buprenorphine
C. Heroin will have both a greater efficacy and a lower ED50 compared to buprenorphine
D. Heroin will have both a greater efficacy and a greater ED50 compared to
buprenorphine
E. Heroin will have a greater therapeutic index compared to buprenorphine
78. W.G. is a 44-year-old female patient who has been treated for 2 months with
C
propranolol
to help lower her blood pressure. She complains of experiencing nightmares
which began shortly after starting the propranolol treatment. She is told to immediately
stop taking the propranolol. Indicate which of the following consequences/explanation
are the most appropriate to describe the results of an abrupt stopping of the propranolol
treatment:
A. Continued drop in blood pressure/Due to loss of alpha1 receptors on vascular smooth
muscle
B. Continued drop in blood pressure/Due to loss of beta1 receptors in the heart
C. Heart palpitations/Due to increased number of beta1 receptors in the heart
D. Bronchoconstriction/Due to loss of beta2 receptors in the lung
E. Bradycardia/Due to increased number of muscarinic receptors in the heart
79. Which drug blocks L-type calcium channels, as its major mode of action?
D
A. procainamide
B. quinidine
C. disopyramide
D. verapamil
80. Which drug is most likely to cause marked prolongation of the QT interval, and polymorphic ventricular tachycardia (torsade de pointes)?
A. sotalol
A
B. diltiazem
C. verapamil
D. propranolol
81. Drugs that have as their primary effect
slowing of conduction and prolongation of refractoriness in atrial and
ventricular muscle include all of the following, except:
A. procainamide
C
B. flecainide
C. digitalis
D. quinidine
_____________________________________________________________________
 Questions 82 – 84 pertain
to the diagram to the left. A normal
patient has a baseline pressure-volume loop labeled "Baseline".
Questions 82 – 84 pertain
to the diagram to the left. A normal
patient has a baseline pressure-volume loop labeled "Baseline".
82. The pressure-volume loop labeled "X" might be generated by:
a. giving volume
b.
A
giving an ACE-inhibitor
c. giving a diuretic
d. giving an inotropic agent
83. The pressure-volume loop labeled "Y" might be generated by:
a.
B
giving volume
b. giving an ACE-inhibitor
c. giving a diuretic
d. giving an inotropic agent
84. The distance "Z" (shown by
the labeled double arrow) represents:
a.
D
cardiac output
b. preload
c. afterload
d. stroke volume
e. end-systolic volume
An 82 year old female with a long standing history of a “heart murmur” presents to the ER with acute shortness of breath and palpitations. Physical exam reveals:
Pulse 120, irregularly irregular; BP: 150/60; Resp: 28, rapid
Neck: Increased JV pressure to ~ 20 mmHg
Chest: Rales 1/3 the way up
Heart: Irregular S1 and S2 with a III/VI diastolic decrescendo blow at the left sternal border; an S3 gallop is present
85. Her irregular heart rhythm most likely is due to:
-
sinus tachycardiaE
- frequent ventricular premature beats
- ventricular tachycardia
- torsades des pointes
- atrial fibrillation
86. Her predominant valvular abnormality is:
A.
B
aortic stenosis
B. aortic insufficiency
C. mitral stenosis
D. mitral insufficiency
E. Pulmonic insufficiency
87. Her left ventricle suffers from:
A.
B
chronic pressure overload
B. chronic volume overload
C. acute pressure overload
D. acute volume overload
E. acute coronary ischemia
88. Medical therapy for her dyspnea and palpitations might include:
A.
E
Digoxin to slow her heart rate
B. Diuretics to reduce preload
C. ACE-inhibitors to reduce preload and afterload
D. Arterial vasodilators to reduce afterload
E. All of the above
89. This patient’s heart may be subject to all of the following, except:
-
DecreasedA
- Increased
- Increased
- Increased
- Decreased diastolic blood pressure, decreasing myocardial oxygen supply