Bio-Med
Combined
Cardiac Pathophysiology,
Pharmacology &
Pathology Exam
September
27, 2005
Course Directors:
| Pharmacology |
Pathophysiology | Pathology |
| Robert Patrick, Ph.D. |
Douglas Burtt, M.D. | Calvin E. Oyer, M.D. |
| Hank Wu, M.D. |
Wisdom begins in
wonder
Socrates
Questions 1 – 4: A 45
year old white male develops shaking chills and a fever to 103 degrees, several
days after being diagnosed with a tooth abscess. He has no prior history of
heart murmur or rheumatic fever. Several days later, he develops progressive
shortness of breath and is unable to lie flat in bed. He presents to the
emergency room, where physical exam reveals the following:
Vital signs: Pulse: 120,
regular Blood
pressure: 120/80 Resp
rate: 24 Temp: 103.5° F.
Neck: 5 cm JVD with
normal upstrokes, no bruit
Chest: Rales ½ the
way up bilaterally
Cardiac:
Abdomen: Benign
Extremities: No edema
1. The
most likely primary valvular abnormality present is:
a)
Aortic
stenosis
b)
Acute
aortic insufficiency
c)
Chronic
aortic insufficiency
d)
Acute
mitral regurgitation
e)
Chronic
mitral regurgitation
2. A likely
diagnostic finding at right heart catheterization in this patient would be:
a)
Rapid
y descent in the right atrial tracing
b)
Oxygen
saturation step-up between the right atrium and the pulmonary artery
c)
Large
V-waves in the pulmonary capillary wedge tracing
d)
Large
V-waves in the right atrial tracing
e)
Equalization
of diastolic pressures in the LA,
3. Administration of
an ACE-inhibitor in this patient would:
a)
decrease
preload alone
b)
decrease
afterload alone
c)
decrease
both preload and afterload
d)
decrease
heart rate by a negative chronotropic effect
e)
decrease
stroke volume
4. Shortly after
admission to the hospital, the patient’s condition worsens. His blood pressure
drops to 80/60 and his heart rate rises to 130/minute. Treatment of this
patient might include all of the following, except:
a)
insertion
of an intra-aortic balloon pump to decrease afterload and improve coronary
blood flow
b)
administration
of intravenous antibiotics to treat infection
c)
consideration
of urgent surgery to replace his heart valve
d)
administration
of Verapamil to lower his heart rate
e)
administration
of a positive inotropic drug to improve myocardial contractility
5. Dobutamine is sometimes used to treat patients with congestive heart failure. Dobutamine works by stimulating:
a) the beta 1 receptors in the heart to increase intracellular Cyclic AMP levels
b) the beta 2 receptors in the heart to increase intracellular levels of Inositol triphosphate (IP3)
c) the dopamine receptors in the heart to stimulate the intracardiac Na+-Ca+2 exchange
d) Inositol triphosphate receptors to raise intracellular Cyclic GMP levels
e) the alpha receptors in the heart to release Atrial Natriuretic Peptide (ANP)
Question
6- 8: A 72-year-old male with
long-standing hypertension has an echocardiogram, which demonstrates concentric
left ventricular hypertrophy with normal systolic function, and impaired
diastolic filling. His electrocardiogram shows normal sinus rhythm.
6. This patient's "compensatory" left
ventricular hypertrophy:
- Increases wall
tension (wall stress)
- Decreases wall tension
- Increases afterload
- Increases preload
- Decreases myocardial
oxygen demand
7. If this patient's
rhythm changed to atrial fibrillation, there would be loss of the "atrial
kick", which might cause a 10 – 30% fall in cardiac output. This
"atrial kick" occurs:
- Immediately before
opening of the mitral valve
- Immediately after
opening of the mitral valve
- Immediately before
closure of the mitral valve
- Immediately after
closure of the mitral valve
8. This
patient's myocardial oxygen demand might be increased because of:
- Decreased
contractility from left ventricular hypertrophy
- Increased
contractility from left ventricular hypertrophy
- Decreased wall
tension from left ventricular hypertrophy
- Increased wall
tension from left ventricular hypertrophy
***********************************************************************
9. A patient's pulmonary capillary wedge
pressure generally reflects the patient's left ventricular end-diastolic
pressure. Which valvular abnormality would make the pulmonary capillary wedge
pressure significantly higher than the true left ventricular end-diastolic
pressure?
- mitral stenosis
- mitral insufficiency
- pulmonic stenosis
- tricuspid stenosis
- aortic
insufficiency
Question 10- 12: The cross section of a heart illustrated below is from a patient who entered the hospital after experiencing severe chest pain. He subsequently died.

10. The age of the lesion is consistent with:
a) 3 weeks
b) 6 weeks
c) 8 hours
d)
6 days
11. The lesion is in what location?
a) inferolateral (posterolateral)
b)
right
ventricular
c)
anteroseptal
d)
strictly
anterior
e)
strictly
posterior
12. Coronary artery occlusion was probably present in which location?
a) right coronary artery
b)
left
anterior descending coronary artery
before branching of the first diagonal and first septal branches
c)
left
circumflex coronary artery in a patient with left dominant coronary circulation
d)
left
anterior descending coronary artery after branching of the second diagonal and
second septal branches
e) posterior descending coronary artery
Question 13 – 17: A 60-year-old male patient presents with a history of palpitations, shortness of breath on exertion, and fatigue. The patient indicates that his palpitations are felt as irregular heartbeats, occasionally rapid, and sometimes associated with lightheadedness. An electrocardiogram is obtained and lead II is shown below:

13. The
electrocardiogram shows:
a) atrial fibrillation
b) torsades des pointes
c)
mobitz II heart block
d) ventricular tachycardia
14. This patient's
arrhythmia has been shown to do all of the following, except:
a)
be present in up to 5% of adults over 65 years of age
b)
occur more frequently in patients with dilated atria
c)
respond to drugs which slow A-V node conduction,
causing a reduction in heart rate
d) cause an increase in cardiac output, due to loss of atrial kick
e)
predispose to intra-cardiac thrombi, which may lead to
thrombo-embolism
15. Digoxin is given to the patient to control his rhythm. Digoxin also has a positive inotropic effect on cardiac tissue through:
a) activation of the Na+-K+ ATPase in cardiac myocytes.
b) inhibition of the Na+-K+ ATPase in cardiac myocytes.
c) inhibition of the Na+-Ca+2 Exchanger in cardiac myocytes.
d) inhibition of the Na+-Ca+2 ATPase in cardiac myocytes.
e) activation of the Na+-Ca+2 ATPase in cardiac myocytes.
16. Which of the following conditions is most likely to predispose to digoxin toxicity?
a)
Hyperkalemia
b)
Hypokalemia
c)
Hypermagnesemia
d)
Hypocalcemia
e)
Concomitant
use of antibiotics
17. The major antiarrhythmic actions of digitalis are due to:
a) Sympathetic blockade
b) Inhibition of the Na/K ATPase pump
c) Parasympathomimetic actions
d) Improvement in ventricular function resulting from its positive inotropic effects.
18. Activation of cells in the AV node occurs primarily as a result of transmembrane movement of calcium ions because:
a) Neighboring atrial myocytes exert electronic influence on the AV nodal cells.
b) The cells of the His bundle conduct electrical impulses extremely rapidly.
c) The resting membrane potential of AV nodal cells is approximately negative 60 mV.
d) The resting membrane potential of His bundle cells is approximately negative 90 mV.
19. The response of the action potential of working ventricular myocytes to change in stimulation rate is best described as:
a) Increasing rates shorten the action potential duration.
b) Increasing rates prolong the action potential duration.
c) In contrast to Purkinje cells, working ventricular myocytes show little change in action potential duration when stimulation rates change.
d) Increasing the stimulation rate abbreviates the action potential duration only in the presence of hypokalemia.
20. The most common mechanism causing pathologic cardiac tachycardias in people who hearts are structurally normal (as opposed to persons who have experienced a myocardial infarction) is:
a) Automaticity
b) Triggered activity due to early afterdepolarizations
c) Triggered activity due to delayed afterdepolarizations
d) Reentry
21. Prolongation of the action potential of working ventricular myocytes is most likely to facilitate arrhythmias due to:
a) Abnormal automaticity resulting from myocardial ischemia
b) Intramyocardial reentry following myocardial infarction
c) Triggered activity resulting from early afterdepolarizations.
d) None of the above.
22. Which of the following agents should never be used to treat atrial fibrillation in a 50 year old man who experienced myocardial infarction 5 years previously:
a) Digitalis
b) Verapamil
c) Dofetilide
d) Flecainide
Questions 23 – 26: A 40 year old woman was experiencing exertional dyspnea, orthopnea and paroxysmal nocturnal dyspnea. Though her heart disease was problematical, her death was due to an auto accident. The photo below is of her open left atrium and ventricle. Note the status of the left atrioventricular valve and of the chordae tendineae.
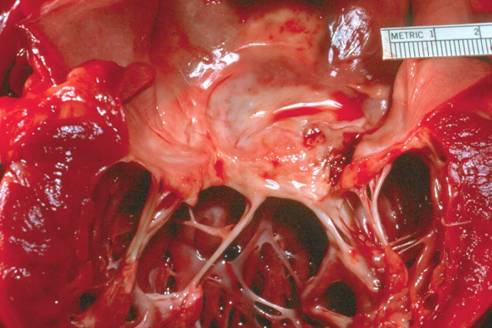
Are the following statements A true or B false?
23. It is probable that several years previously the patient had pharyngitis followed by a febrile illness with dyspnea and cardiomegaly.
24. It is probable that the patient has Marfan syndrome.
25. It is extremely unlikely that the left semilunar valve is also involved.
26. The first symptoms/signs of patients with this abnormality are related to right ventricular failure.
***********************************************************
Match the entity A or B with the following descriptions/events.
- Viral myocarditis
- Hypersensitivity myocarditis
27. All chambers of
heart dilated; interstitial infiltration with abundant inflammatory cells,
predominantly eosinophils; foci of myocyte necrosis.
28. All chambers of
heart dilated; interstitial infiltration with abundant inflammatory cells,
predominantly lymphocytes; foci of myocyte necrosis.
29. Can occur in utero and may cause endocardial fibroelastosis.
30. Can follow
administration of commonly used medications such as ampicillin.
Question 31 – 35: A 48 year old man had poorly-controlled hypertension for several years and then died suddenly from a massive cerebral hemorrhage.
31. The heart image
in the center above is normal. Which heart image would a cross-section of the
heart of this man be likely to resemble, A
the left image or B the right
image?
32. The adaptive process secondary to his hypertension is called:
a) dilated cardiomopathy
b)
eccentric
hypertrophy
c)
concentric
hypertrophy
33. The left image is likely to result from:
a) pressure overload
b)
volume
overload
34. The right image is likely to result from:
a) pressure overload
b) volume overload
35. Which of the following illnesses is likely to result in a heart consistent with the image on the right?
a) mitral stenosis
b) coarctation of the aorta
c) aortic valve regurgitation
d) tricuspid regurgitation
PHARMACOLOGY QUESTIONS (36- 49):
36. The percentage of a given receptor population that is occupied by a drug can be calculated from which of the following parameters?:
a)
Drug
concentration and dissociation constant
b) Drug concentration and receptor concentration
c) The association and dissociation rate constants
d) Potency and efficacy
e) The therapeutic index and therapeutic window
37. Indicate which of the following is correct:
a) In selecting a drug, potency is usually more important than efficacy
b) The greater the efficacy, the greater the potency of a drug
c)
A
competitive antagonist increases the ED50 for a drug
d) A partial agonist always has lower potency than a full agonist
e) If 10 mg of drug A gives the same response as 100 mg of drug B, drug A is more efficacious than drug B
38. Variability among individual patients in their response to a given drug is most important:
a) Always
b)
When
the therapeutic index is low
c) When the therapeutic index is high
d) When the potency is low
e) When the potency is high
39. Histamine causes contraction and narrowing of the bronchial tree while epinephrine causes the muscles to relax. The action of epinephrine in opposing the action of histamine is due to:
a) Noncompetitive antagonism
b) Competitive antagonism
c) Partial agonism
d) Tachyphylaxis
e)
Functional
antagonism
40. A definition of the therapeutic index of a drug:
a) The lethal dose50 (LD50) divided by the toxic dose50 (TD50)
b) The effective dose50 (ED50) divided by the TD50
c)
The
TD50 divided by the ED50
d)
The ED50 divided by the LD50
e) The ED50 minus the TD50
41. Which of the following statements is correct regarding the autonomic nervous system?
a) The sympathetic nervous system arises primarily from craniosacral outflow tracts
b) The division of the autonomic nervous system activated in response to emotional and physical stress is called the parasympathetic nervous system
c)
The
primary catecholamine released by chromaffin cells in
the adrenal medulla is epinephrine
d) Nicotine is the neurotransmitter released by preganglionic neurons
e) The neurotransmitter released by postganglionic parasympathetic neurons is norepinephrine
42. Cocaine can cause a dose-dependent increase in heart rate. By what mechanism does it cause this action?
a) Increased synthesis of norepinephrine from epinephrine in the postganglionic neuron
b) Decreased release of norepinephrine from storage vesicles in the postganglionic neuron
c) Increased release of norepinephrine from the postganglionic neuron by diffusion
d)
Decreased
reuptake of norepinephrine into the postganglionic neuron from the synaptic
cleft
e) Direct stimulation of cardiac catecholamine receptors
43. Which of the following statements is correct?
a) Epinephrine is more potent than norepinephrine at stimulating beta-1 receptors
b) Norepinephrine is a better choice than epinephrine in treating an asthmatic patient because it is more potent at stimulating beta-2 receptors
c) Dobutamine is the precursor for norepinephrine synthesis
d) Both norepinephrine and epinephrine can be administered orally
e)
Dopamine's
renal vasodilatory properties are produced at lower
dosages than those that produce general vascular constriction
44. Doxazosin and terazosin are both commonly used drugs for the treatment of hypertension and benign prostatic hyperplasia. Which of the following actions account(s) for this benefit?
A. Alpha-1 receptor blockade
B. Alpha-1 and alpha-2 receptor blockade
C. Muscarinic receptor blockade
D. Nicotinic receptor blockade
E. Alpha-2 receptor stimulation
45. A patient is receiving an oral beta-blocker following discharge from the hospital for a myocardial infarction. The goal is to keep his resting heart rate between 55 and 60 beats per minute as well as to maintain a reduced heart rate during exercise. Based upon this information, which of the following drugs is LEAST appropriate for this patient?
A. Metoprolol, a beta-1 selective beta-blocker
B. Propranolol, a non-selective beta-blocker with membrane stabilizing activity
C. Carvedilol a non-selective beta-blocker with additional alpha-1 blocking effect
D. Pindolol, a non-selective beta-blocker with intrinsic sympathomimetic activity (ISA)
46. Which of the
following statements regarding the cholinergic system is correct?
A. Acetylcholine is the transmitter released by
postganglionic sympathetic neurons
B. The most important mechanism for removal of acetylcholine
from the synaptic cleft is enzymatic metabolism
C. Stimulation of the M2 muscarinic receptor in the heart leads to increased myocardial contractility
D. Administration of methacholine is likely to produce bronchodilation in a patient with asthma
E. Only two muscarinic receptor types (M1 and M2) are known to exist in humans
47. A 70 year-old man has slowing of conduction in his atrioventricular (AV) node resulting in a significant reduction in his ventricular rate and hypotension. Given this information, which of the following medications would be most appropriate for this patient?
A. Acetylcholine
B. Pyridostigmine
C.
Atropine
D.
Ipatropium
E.
Pilocarpine
48. Parasympathomimetic drugs are categorized as either direct-acting or indirect-acting. Which of the following statements is correct?
A. Pilocarpine is an example of an indirect-acting parasympathomimetic drug
B. A direct-acting parasympathomimetic drug works by directly blocking the muscarinic receptor on the target organ
C. An indirect-acting parasympathomimetic
drug works by decreasing the breakdown of acetylcholine
D. Donepezil (Aricept) is an example of a direct-acting parasympathomimetic drug
E. Both direct- and indirect-acting parasympathomimetic drugs are approved for the treatment of gastrointestinal hypermotility
49. Mr. Mucho Regurgitation has recently had a successful mitral valve replacement operation for severe mitral regurgitation. His echocardiogram 3 months after his open-heart surgery showed a good functioning prosthetic mitral valve, but an enlarged left ventricle with an ejection fraction of 35% and global hypokinesis. He does not complain of any symptoms of heart failure, and is walking daily with a very good functional status. Which of the following drugs would be expected to have the SMALLEST or NO benefit on his heart’s long term systolic function?
A. Carvedilol
B. Enalapril
C. Digoxin
D. Lisinopril
E. Sustained
Release Metoprolol
The following questions (50 – 55) are TRUE (A) or FALSE (B):
Left ventricular end diastolic pressure (LVEDP) is elevated in:
50. hypertrophic cardiomyopathy
51. dilated cardiomyopathy
52. restrictive cardiomyopathy
53. mitral stenosis
54. acute myocardial infarction
55. isolated right ventricular infarction
Questions 56 – 59:
You are treating a 50 year-old male diaphoretic businessman who was brought to the emergency room with chest pain. He looks pale, anxious and apprehensive. His heart rate is 45 beats/min (normal 60-100 beats/min) and his blood pressure is 80/40 mm Hg (normotensive >90/60). Immediate EKG showed inferior ST segment elevations. His right-sided EKG showed ST elevation in leads V4-5 suggestive of infarct.
56. Which of the following immediate actions would be most appropriate?
A. IV nitroprusside sodium after arterial line placement
B. IV fluids – normal saline
C. IV beta-blockers
D. IV enalapril
E. IV digoxin
57. The cause of his low resting heart rate could be any of the following, except:
A. increased vagal (parasympathetic) tone
B. ischemia of the sino-atrial (SA) node, causing sinus bradycardia
C. ischemia of the AV node, causing Mobitz I (Wenckebach) 2nd degree block
D. ischemia of the AV node, causing 3rd degree AV block with a junctional escape rhythm
E. ischemia of the His-Purkinje system, causing left bundle branch block
WRITE IN YOU NAME HERE: __________________________________________________
58. This patient’s myocardial infarction is most likely due to a ruptured atherosclerotic plaque. When
a plaque ruptures, thrombosis is likely to occur when blood is exposed to thrombogenic substances in
the _________________ ______________ of the atherosclerotic plaque.
59. When we say that a plaque ruptures, we really are talking about rupture
of the________________ _____________of the atherosclerotic plaque.
Question 60 – 62: The photo below is from a 37 year old woman with Turner syndrome. She had a bicuspid aortic valve and aortic root dilation. Death was sudden. The pericardial sac was distended with blood under pressure.
Fill in the blanks:
60. The condition in the aorta which resulted from entry of blood into the media via the intimal tear is
called _________________ __________________.
61. When death is caused by the presence of blood or other fluid under pressure in the pericardial sac
we call that condition ________________ ___________________.
62. If the condition in the previous question occurs as a result of myocardial rupture, how much time is likely to have elapsed following coronary occlusion?
A 12-24 hours, B 2-3
days, C 4-7 days, D 11-14 days, E 3 weeks
63. You are treating a patient for
chronic stable angina and wish to use a coronary vasodilator. Which of the
following lists of three drugs are all coronary vasodilators?
A. Nitroglycerin, propranolol, nifedipine
B. Propranolol, nifedipine, amlodipine
C. Nifedipine, isosorbide dinitrate, atenolol
D. Nifedipine, nitroglycerin,
amlodipine
64. Tolerance to anti-anginal effectiveness has been observed most commonly among
which group of drugs?
A. Calcium antagonists
B. Organic
nitrates
C. Beta-blockers
D. Direct anti-thrombins
65. Indicate which of the following statements concerning nifedipine is correct:
A. It has a
greater effect on arteriolar vasodilation compared to its effect on cardiac
conduction
B. It is likely to produce reflex bradycardia
C. It is contraindicated (not to be used) for the treatment of angina caused by spontaneous
coronary spasm
D. It blocks both alpha-1 and alpha-2 catecholamine receptors
66. Which of the following drugs used for acute coronary syndromes requires antithrombin-3 for its therapeutic effectiveness?
A. Abciximab
B. Lepirudin
C. Aspirin
D. Ticlopidine
E. Heparin
Questions 67 – 69: The following questions are TRUE (A) or FALSE (B):
67. Microscopic polyangiitis is a small vessel arteritis
in which normal neutrophils exposed to the patient’s
serum show positive staining of perinuclear antineutrophilic cytoplasmic
antibodies.
68. Kaposi sarcoma
occurs in about one-third of AIDS patients, especially homosexual men and about
one-third of the affected patients will develop lymphoma.
69. Dressler syndrome (post-myocardial infarction syndrome) is
caused by autoimmunity but postpericardiotomy
syndrome is usually on the basis of a retained sponge or other surgical
misadventures.
Questions 70 – 76: This heart is that of a 22 year old man who died suddenly. There was a family history of early sudden cardiac death.
70. Which of the following genetic defects might have been present?
A a deletion on the long arm of chromosome 22
B absence of the homeobox gene, tinman
C a mutation in the b- myosin heavy chain gene
D faulty timing
of expression of the Sonic hedgehog gene.
71. Which of the following histological features is likely to be seen in sections of the left ventricular myocardium?
A myofiber disarray
B dense interstitial infiltration with lymphocytes
C an apparent decrease in nuclear DNA as judged by size and staining of nuclei
D nuclear inclusions indicating a viral infection
72. What type of heart murmur would this patient be likely to have:
A. A systolic ejection murmur and a diastolic decrescendo blowing murmur
B. An opening snap and a diastolic rumble with presystolic accentuation
C. A mid-systolic click followed by a late systolic apical murmur
D. An early-peaking systolic ejection murmur accentuating with Valsalva
E. A late-peaking systolic ejection murmur with delayed carotid upstrokes
73. Which of the
diastolic filling curves below would most likely represent this patient’s
A. The upper curve
B. The lower curve
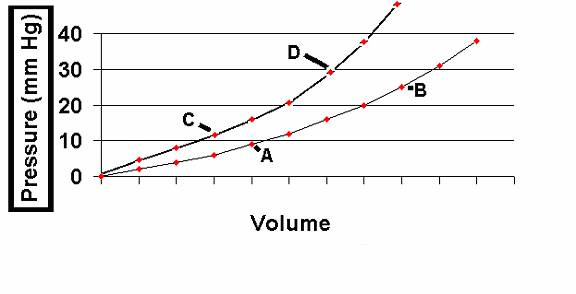
74. If this patient presented with congestive heart failure, at which point on these curves would he most likely be?
A. Point A
B. Point B
C. Point C
D. Point D
75. Giving this patient a beta-blocker over a period of time would likely:
- Move him from point A to point B
- Move him from Point B to point A
- Move him from point D to point C
- Move him from the upper curve to a lower curve
- Move him from the lower curve to a higher curve
76. Left ventricular compliance is measured as the:
- Reciprocal
of the slope of the
- Slope
of the
- Wall
tension of the
- Wall
tension of the
Question 77 : You are asked to see a 58 year-old male contractor in consultation. During your office evaluation, he stated that aside from having one or two mild episodes of asthma over the last few years he was well until 2 months ago when he began to experience chest discomfort while walking. The discomfort is described as a fullness or pressure-like sensation. If he stops walking, the sensation disappears. He has not experienced this discomfort while at rest. His primary care physician had an exercise stress test performed that demonstrated ST-segment depression with exercise as well as the chest discomfort. His only medication is an inhaler for his asthma that he uses rarely. On physical exam his heart rate was 84 bpm and blood pressure 140/85 mmHg. His lungs were clear and his cardiac exam normal.
77. Which of the following medications would be the most suitable to initiate for this patient?
A. Nitroglycerin patch during day time hours and oral propranolol
B. Oral isosorbide mononitrate and oral propranolol
C. Nitroglycerin patch during daytime and evening hours and oral amlodipine
D. Oral isosorbide mononitrate and
oral metoprolol
E. Nitroglycerine patch during daytime and evening hours and oral metoprolol
78. Which of the following agents acts by ADP-receptor blockade?
A.
Clopidogrel
B. Lepirudin
C. Bivaliudin
D. Aspirin
E. Eptifibatide
79. Eisenmenger’s syndrome occurs when:
a. A congenital membranous VSD spontaneously closes around 12 months of age
b.
RV compliance exceeds
c. Atrial fibrillation occurs in Tetralogy of Fallot
d. Pulmonary hypertension from the chronic shunt overload leads to right-to-left shunting
e. A cleft mitral valve occurs in association with a VSD
80. A factor common to all Class I ((Vaughan Williams) drugs is:
A. Their property of blocking the rapid inward sodium current.
B. Their property of blocking the slow inward sodium current.
C. Their property of blocking the rapidly activating outward potassium current.
D. Their property of blocking the slowing activating outward potassium current.
E. Their property of blocking the slow inward calcium current.
81. Amiodarone is unique among currently available antiarrhythmic agents in that:
A. It has properties common to all 4 Vaughan Williams classes.
B. It is the only available drug that blocks the IKs current.
C. It is devoid of side effects.
D. Its onset of action is extremely rapid – within seconds.
Questions 82 – 87: The following diagram depicts jugular venous pressure tracings in a normal individual (diagram A), and in two patients with pericardial disease (B and C). Please answer the True/False questions below, based on this diagram:
Answer True or False (A = True, B = False):
82. The patient depicted in panel B may have pericardial tamponade, based on the blunted y-descent shown
83. The patient in panel B is likely to exhibit elevated overall jugular venous pressure.
84. The patient in panel B is likely to exhibit pulsus paradoxus.
85. The patient in panel C may have pericardial constriction, based on the rapid y-descent.
86. The patient in panel C is likely to exhibit elevated overall jugular venous pressure.
87. The patient in panel C is likely to exhibit pulsus paradoxus.
88. Left ventricular preload is defined as:
a) The amount of volume filling the left ventricle
b) The
c) The
diastolic wall radius of the
d) The
e) The
sum of rapid ventricular filling and the left atrial "kick"
Questions 89 – 91: A normal patient has a pressure-volume loop shown below (labeled "Baseline").
89. The pressure-volume loop labeled "X" might be generated by:
a. giving volume
b. giving an ACE-inhibitor
c. giving a diuretic
d. giving an inotropic agent
90. The pressure-volume loop labeled
"Y" might be generated by:
a. giving volume
b. giving an ACE-inhibitor
c. giving a diuretic
d. giving an inotropic agent
91. The distance "Z" (shown by
the labeled double arrow) represents:
a. cardiac output
b. preload
c. afterload
d. stroke volume
e. end-systolic volume