Cortical adrenal adenoma
28 year old female presented with a history of hypokalemia and hypertension. CT of the abdomen showed a 2.4 cm mass of the left adrenal and normal right adrenal. The patient underwent left adrenalectomy.

Grossly the adrenal appeared normal sized, with a 2.0 cm nodule seen compressing adjacent normal adrenal. The cut surface of the lesion was golden yellow.
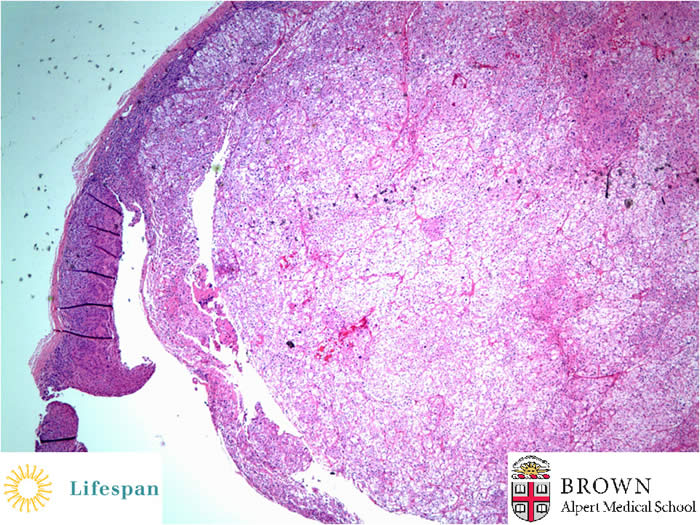
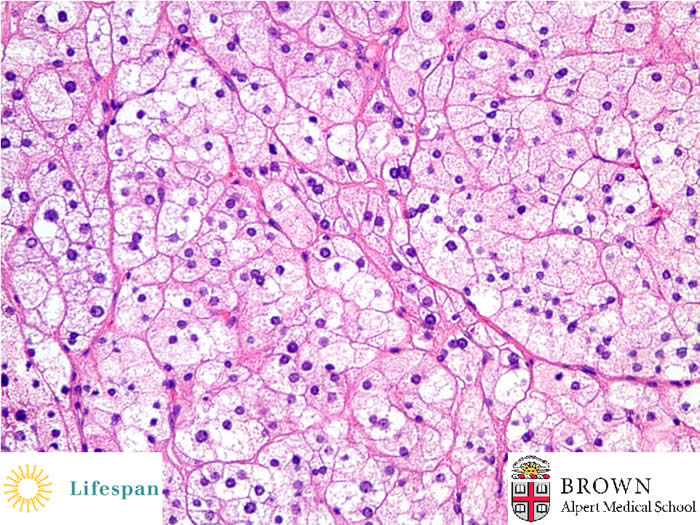
Microscopically, the nodule appeared to arise from the cortex, with compression of a rim of normal adrenal tissue. The cells of the nodule were large, clear cells with characteristic microvesicular cytoplasm, mimicking the zona fasciculata of the normal adrenal. There were no spironolactone bodies (eosinophilic whorled, intracytoplasmic inclusions) identified.
Clinically, the lesion was compatible with an aldosteronoma.
The main causes of primary hyperaldosteronism (Conn’s syndrome) are cortical hyperplasia, cortical adenoma and familial hyperaldosteronism. No consistent genetic changes have been identified to characterize cortical adenomas. Inherited syndromes that are associated with adrenal cortical adenomas include Carney complex (myxomas of multiple organs and skin hyperpigmentation), multiple endocrine neoplasia type 1 and McCune-Albright syndrome.
Contributed by Sonja Chen, MD