Influence of
area MT on Smooth Pursuit (view
Landscape)
Reading: You will have a copy of W. Newsome,
R. Wurtz, M. Dursteler & Mikami, (1985), "Deficits in visual motion
processing following ibotenic acid lesions of the middle temporal visual area
of the macaque monkey", J. Neurosci 5: 825-840. link
to the paper online, when on brown.edu.
Link to my (archive) review of paper.
MT is the medial temporal area of cerebral cortex, a region of direction-selective
cells.
In the Newsome experiment there are two regions of retina to consider: the periphery,
where the target jumps to as it starts moving, and the fovea, where the SP
system will try to hold the target as it moves. It is the region of MT that represents
the periphery that is lesioned by 1 micro-liter of ibotenic acid.
Fovea
vs Periphery: The
1 μL ibotenic acid injection kills cells, but not fibers of passage, in a localized
area. Newsome et al. lesioned cells that monitor visual space along the horizontal
meridian.

To begin with, the macaque is foveating, so the target is arranged to appear in
the region where the lesion occurred. You will want to appreciate the fovea and
the periphery (where the injection occurs) as 2 paths in the model. There will be
a diminished response to the target starting to move in the space mapped by lesioned
area.
Requirements:
From c:\MatlabR12\work\fold22 you can find read-only simulink model asgn12B05D.
Copy and rename the model in your IP folder.
Notice provisions are made in the model for peripheral movement detection.
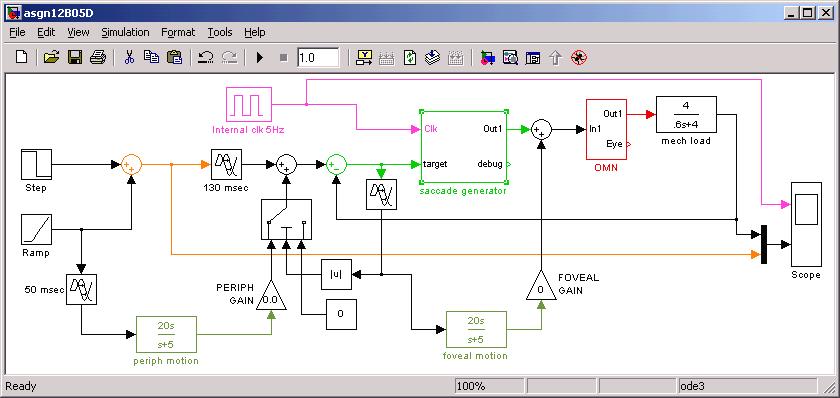
The input on the left is a
step + ramp. They combine and are taken to the scope. Next is a 130 msec "saccade
visual delay" then a pathway to the saccade
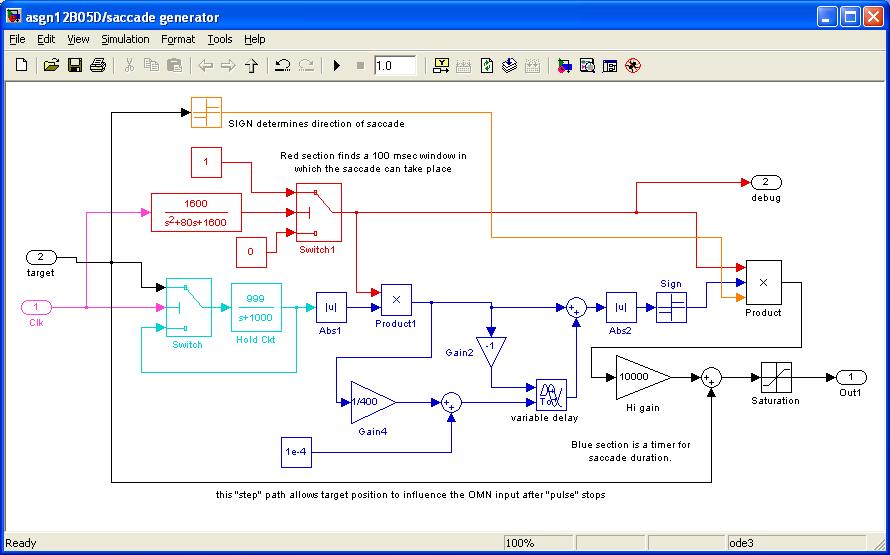
generator subcircuit. The saccade generator here does not require EYE feedback
from the OMN; it "computes" a saccade pulse duration. The saccade
generator combines the pulse with target position ("step" part of
the pulse-step control).
The ramp only goes to motion detectors
for the periphery and the fovea. The PERIPH detector feeds into the saccade generator
input, while the foveal motion detector adds directly to the OMN input.
(1) Control experiments: Run
the distribution model to see a response to step-down+ramp target, where the
Periph Gain is v. low and the saccade response overshoots the correct response.
Now set the motion detector
gains to zero and the ramp slope to zero. Test that the model makes correct
saccades to either left or right (+/- 10 deg) saccades. Let your simulation
run for 2 seconds, with max step size of 2 msec.
(1b) Turn off the step input
and turn on the ramp, to 15-30 deg/sec. How does the eye follow the stimulus?
What if you make saccade output always zero, what minimal gains must be set
to have the eye to follow the stimulus SPEED?
(2) Now try to reproduce Fig
3 and Fig 9 of Newsome et al., showing that if the peripheral gain is zero the
saccade under- or over-reaches the moving target.
(3) What happens if you have
a step + ramp, as shown below?
Arrange that you can form a step + ramp target that is reached (by the "uninjured"
model) with no saccade at all.
(BONUS: no
FTQ) Newsome et al.
say that function recovers in a few days, in spite of the lesion. While Newsome
did not acknowledge the work of Robinson in highlighting the role of the cerebellum
for correcting visuomotor mistakes, investigate (like you did for Gain Mod and
Sacc Dysmet asgn's) recovery here. Say the perceived speed detection after lesion
is 10% of what it should be. Show a "recovery" mechanism that monitors
the error of initial SP and corrects the problem by increasing a downstream
gain. Let's say the correction must occur at a site different from the lesion.
To begin with, make a "manual" adjustment to show the site of change.
Possible FTQ's: How
can you add 50 msec of motor delay to the saccade path? Explain how the saccade
pulse duration can be generated in Simulink.
{kind=link}