









Determining the appropriate level of intervention for an adolescent is no small task. In addition to factors normally considered when intervening or treating an individual for a substance use problem, such as severity of substance use, cultural background, and presence of co-existing disorders, interventions must also examine variables such as age, level of maturity, gender, family and peer environment. Once these factors are identified and the severity of the problems assessed, the intervention can be defined to most effectively address the adolescent’s needs.
Research has established clinical screening for alcohol and other drug problems as a valid and necessary standard of care in a variety of settings, including emergency departments, trauma centers, primary care, pediatrics, family practices, and the justice system. The most commonly used and validated screening method is confidential questioning or interviewing of adolescents and/or their parents. Most methods rely on self-report, which is generally valid, but not always perfect, so obtaining collateral information is important. Because adolescents are a unique population, screening and assessment instruments have been specifically designed for adolescents. There are several developmentally-appropriate, valid, and reliable screening instruments available to screen adolescents for substance use disorders, including the Adolescents Drug Involvement Scale (ADIS) Drug and Alcohol Problem (DAP) Quick Screen, Global Appraisal of Individual Needs (GAIN) and the CRAFFT. It is important to screen adolescents for both mental health and substance use disorders because the two often co-occur.
CRAFFT Test
The CRAFFT was specifically designed to screen for alcohol and drug problems in adolescents in a health care setting. Rather than asking direct questions about quantities and frequencies of alcohol and drug consumption, it asks 6 questions about behaviors that are reliable indicators of consumption and risk. The CR AFFT is used by the juvenile justice system as a screening instrument with five Reclaiming Futures sites. Reclaiming Futures is an initiative to help communities improve their approaches for working with youth involved in the juvenile justice and treatment systems (www.reclaimingfutures.org).
C Have you ever ridden in a car driven by someone (including yourself) who was “high” or had been using alcohol or drugs?
R Do you ever use alcohol or drugs to relax, feel better about yourself, or fit in?
A Do you ever use alcohol or drugs while you are by yourself, alone?
F Do you ever forget things you did while using alcohol or drugs?
F Do your family or friends ever tell you that you should cut down on your drinking or drug use?
T Have you ever gotten into trouble while you were using alcohol or drugs?
If a screening questionnaire identifies the presence of an alcohol or other drug problem, a clinical assessment should be administered. The assessment is an important link between identifying the problem and treating the problem. Formal clinical assessments can confirm the presence of a disorder, determine the level and severity of the problem, and identify what services and/or treatment would be most effective to treat the problems (Knight et al., 2003).
A behavioral specialist, such as a chemical dependency counselor, social worker, certified addiction counselor, psychologist, or addiction medicine specialist should administer, and interpret results of clinical assessments. Sharing the information gathered from an assessment between the treatment and justice systems is critical. A clinical diagnosis is important to ensure valid information is obtained to identify the needs and risks of individuals and/or their families.
For more information on screening and assessment:
Tools:
www.drugstrategies.com/teens/research.html
See Section 2
Treatment
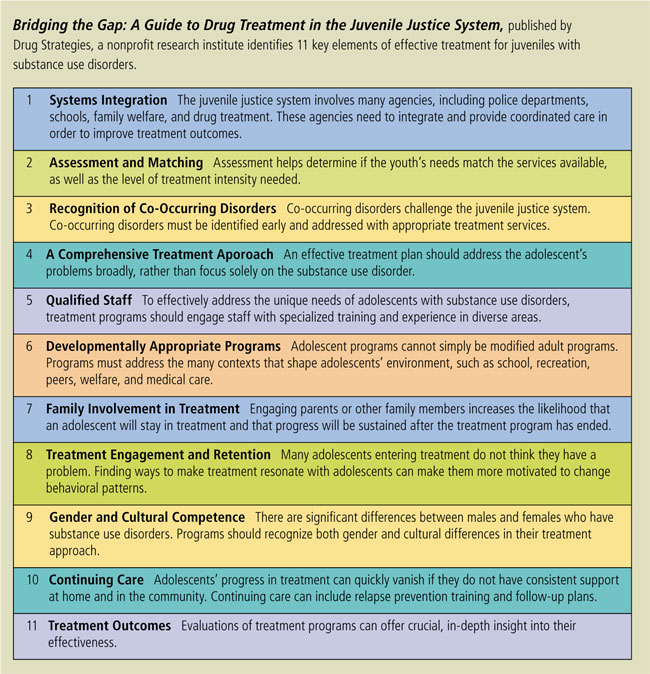
Adolescents present unique challenges to the treatment and justice systems because of the physical, psychological, and developmental changes associated with their age group, in addition to the factors associated with their delinquency. There is no one method of treatment that is most effective for treating adolescents with alcohol and other drug problems. In order to increase successful outcomes, treatment programs should be specifically designed to meet an individual’s short and long term needs.
Knowledge of the needs of treating adolescent substance abuse and defining appropriate treatment continues to increase, and with this knowledge comes a clearer understanding of our shortcomings. While the capacity for treatment continues to grow, only 1 in 10 adolescents receives treatment and, of those who do receive treatment, only 25% receive enough (CSAT). It is imperative to address the lack of treatment availability and evaluate current and new treatment methods to determine their effectiveness in reducing adolescent substance use disorders.
Five Things To Remember About Treatment For Adolescents
- Relapse is common. Most adolescents initiate treatment 2-4 times before they are able to maintain recovery.
- Learn to recognize the signs of relapse (spending time with using friends, breaking rules, staying out, inattention, anger, poor hygiene, declining grades) and get adolescents back into treatment and on the road to recovery right away.
- Helping adolescents participate in continuing care and other recovery support services during the first 90 days after treatment (and ideally the first year) is a key factor in helping them to maintain recovery.
- While treatment is focused on getting an addicted person to stop, self-help groups, recovery schools and other recovery support services are typically designed to help maintain recovery. It is important to try to link adolescents to continuing care services with other adolescents.
- Most adolescents are seen in an outpatient setting several hours a week. Residential treatment is usually reserved for adolescents who are not succeeding in outpatient treatment and/or who have an environment (peers, home) that is making it very difficult for them to stop.
When adolescents do receive treatment, it is most often not evidence-based. Recent research indicates most services in the juvenile justice setting are not provided when an adolescent first becomes involved in the system and do not involve families in the treatment process. Yet even if evidence-based treatment approaches are provided, there is often a lack of cooperation among service providers resulting in fragmented services that are not effective (Young et al., 2007).
While the majority of treatment services are focused on a single episode of care, achieving long-term recovery involves an average of 3 or 4 episodes of care (Dennis et al., 2002). Biological, psychological, psychiatric, and sociological factors interact to influence the risk of relapse for any individual, therefore successful recovery involves the maintenance of new skills and lifestyle patterns that promote positive, independent patterns of behavior. The integration of these behaviors into regular day-to-day activities is the essence of effective relapse prevention. Yet, because adolescents are minors, they do not have the luxury to choose another home, community, or school to return to after treatment and they may have to return an environment that is far from ideal from a relapse prevention perspective.
For more information on determining appropriate evidence-based interventions for the treatment of alcohol and other drug problems:
SAMSHA’s National Registry of Evidence-based Programs and Practices (NREPP)
www.nrepp.samhsa.gov