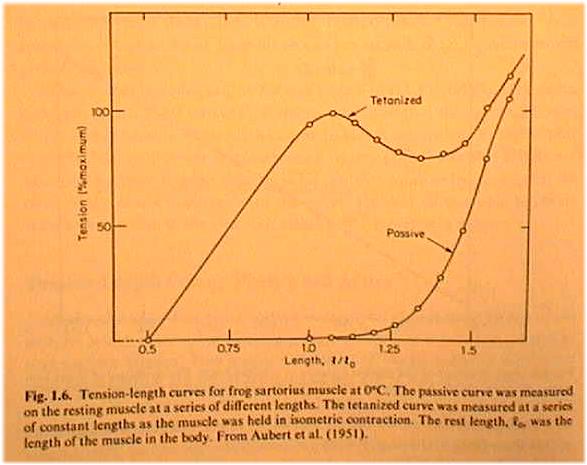
Near L0 the Stress-Strain curve is flatter so the muscle has less stiffness at L0.
After being cut, the stiffness increases. See math involved.
Strabismus surgery
reveiw of John A. Pratt-Johnson & Geraldine Tillson, Management of Strabismus and Amblyopia, Thieme Medical Publishers, New York (1994) RE771.P73, 12th floor Sci Li.
amblyopia: blindness in one eye, Central suppression of vision, due to binocular rivalry (double vision). Can be a result of strabismus, the deviation of one eye's gaze that prevents binocular fusion.
measuring
mismatch of binocular gaze:
Definition: day deviation angle is the mismatch
angle between the gaze of each eye.
then Prism diopters = 100*tan(deviation
angle).
and remember that for small angle thet (in radians) tan thet approx
= thet
since 1 deg = 1/57 radian, then 2 deg prism diopters = 200/57 = 4 diopters
or so
abduction: turning out, lateral gaze
Chpt 1: Development of normal binocular vision.
Chpt
2: What happens if normal development is interrupted?
last section: Social
Implications of Strabismus...
"Living with a
strabismus or having a child with strabismus affects all aspects of
daily
life. For the parents, there is the expense of occlusion, glasses, and visits
to the ophthalmologist's office. Even if they have some kind of insurance,
the
time and costs of transportation involved can be considerable. The endless
questions and advice from family, neighbors, and even strangers in the
supermarket, the teasing that the child has to endure-these all have a major
impact on their lives. When surgery is also needed, this is an additional stress
factor. Adults and older children are frequently asked "Who are you
looking
at?" "Why don't you look at me when you are speaking?"
etc. This makes
social occasions uncomfortable for them because they are
worrying about their
eyes. Applying for a driver's license may involve additional
visits to the
ophthalmologist to have forms completed to show they are fit
to drive even
though they do not have stereopsis. Similarly, a pilot's license
may be denied.
These are just a few of the problems that patients encounter,
particularly if
they have a strabismus without potential fusion ability."
Chpt
3: Looking for Strabismus
"Strabismus and amblyopia
affect approximately 5% of the population.
Amblyopia is the leading cause
of unilateral visual loss in childhood. The
conditions most often requiring
surgery in ophthalmology are cataracts and
strabismus. Amblyopia was the
leading cause of monocular visual loss in the
20 to 70 and older age group,
surpassing diabetic retinopathy, glaucoma,
macular degeneration, and cataract
in the Visual Acuity Impairment Study
sponsored by the National Eye Institute
of the United States. Amblyopia can
be eliminated largely by appropriate treatment
in childhood."
One eye deviates so that binocular single vision
Chpt 4: Sensory evaluation of strabismus
Chpt 5: Motor evaluation of strabismus
Chpt 6: Esophoria, Exophoria and Convergence Insufficiency
"Esophoria
is a convergent strabismus kept LATENT by the presence of bifoveal fusion."
"Esophoria
is prevented from becoming manifest, that is, from becoming an esotropia, by divergence
fusional amplitudes that keep the eyes straight." p. 66.
Chpt
7: Amplyobia: blindness in one eye, not due to problems in the retina:
photoreceptors, glaucoma, macular degeneration...nor to a tumor pressing down
on the optic chiasm, nerve tract. not due to stroke. it's central, suppressed
synapse blindness...
review Hubel & Wiesel, Nobel Prize in 1984?
monocular
occlusion vs dark rearing
strabismus and loss of binocularity
alternating
occlusion and loss of binocularity; what strobe rate?
Chpt
8: Congenital (or Infantile) Esotropia Syndrome (crossed eyes)
not present
at birth--develops over the first 2-3 months.
angle of strabismus usually
in excess of 35 prism diopters = 15 deg, whew.
treatment with prisms. the lady with the tumor on the optic tract.
p99: surgery. not before 6 mo of age, because of spontaneous
improvement.
see viewgraphs in folder
typical: 7mm recession (weakening) of medial rectus. The MR is cut at
its insertion, then held a certain number of mm away by a suture loop sent through
the stump and around through the muscle. The muscle will reinsert where it "dangles"
from the suture, and therefore be weakened.
See Table 16-1 for function of prism diopter correction
needed vs mm of recession.
Near L0 the Stress-Strain curve is flatter so the muscle has less stiffness
at L0.
After being cut, the stiffness increases. See
math involved.
Chpt 9: Acquired Esotropia (crossed eyes)
Chpt 10: Exotropia

Chpt 11:
Chpt 12: The patient with a vertical strabisumus
Chpt 13: Paralytic and paretic strabismus
Chpt
16: General comments on extraocular muscle surgery:
p.
214: problems with the inferior rectus.
Chpt 19: Why does the patient have double vision? Horizontal misalignment too
large to correct with any vergence.
Chpt 20: The patient with nystagmus...